2 Diagnostic Stewardship: Sense or Nonsense?!
Published in Dutch Journal of Clinical Microbiology, 2019 Sep 27, 26:3
(Nederlands Tijdschrift voor Medische Microbiologie; original work in Dutch)
Berends MS 1,2*, Luz CF 2*, Wouthuyzen-Bakker M 2, Märtson AG 3, Alffenaar JW 3, Dik JWH 2, Glasner C 2, Sinha BNM 2
- Certe Medical Diagnostics & Advice Foundation, Groningen, Netherlands
- University of Groningen, University Medical Center Groningen, Department of Medical Microbiology and Infection Control, Groningen, Netherlands
- University of Groningen, University Medical Center Groningen, Department of Clinical Pharmacy and Pharmacology, Groningen, Netherlands
* These authors contributed equally
Abstract
The right test at the right time for the right patient to answer the right questions and start the right treatment - many important decisions have to be made involving multiple medical specialists. The importance of appropriate and timely diagnostics guide this process (stewardship) can be obvious but is still often neglected in classic stewardship concepts of infection management. We describe the approach of a multidisciplinary, intertwined stewardship concept with a focus on diagnostics, where medical specialists in general and microbiologists in particular closely interact for optimal quality of care and patient safety in successful infection management. Diagnostics in medical microbiology laboratories are advancing fast with regards to new technologies and improved workflows. Yet, diagnostics in infection management is broader than this and covers many clinical areas where communication and interaction are the key to make the best use of knowledge and expertise that all specialisms can contribute to patient care. These aspects are demonstrated in two cases of patients with prosthetic joint infections with two very different outcomes.
2.1 Introduction
Diagnostic stewardship or diagnostic stewardship programme (DSP), a trending topic in the field of medical microbiology and beyond. But what is this concept about, is it really so new and how is it incorporated into infection management? The term diagnostic stewardship was used in an opinion piece by Dik et al. which described various facets of infection management, the so-called integrated stewardship [1]. We want to highlight the diagnostic side of this model and describe its concept; diagnostics as a multidisciplinary bigger picture from admission to discharge.
Although the term DSP was first mentioned in an indexed PubMed article in 2016, articles on antimicrobial stewardship (ASP) have been appearing for 15 years (Figure 2.1).
![The increase of articles indexed in PubMed. Search strategies: 'antimicrobial stewardship'[Title/Abstract]; 'diagnostic stewardship'[Title/Abstract]; 'antimicrobial resistance'[Title/Abstract]. Source: https://www.ncbi.nlm.nih.gov/pubmed/ (assessed: 2018-05-31). * Extrapolation based on count from 2018-01-01 to 2018-05-31.](images/02-01.jpg)
Figure 2.1: The increase of articles indexed in PubMed. Search strategies: ‘antimicrobial stewardship’[Title/Abstract]; ‘diagnostic stewardship’[Title/Abstract]; ‘antimicrobial resistance’[Title/Abstract]. Source: https://www.ncbi.nlm.nih.gov/pubmed/ (assessed: 2018-05-31). * Extrapolation based on count from 2018-01-01 to 2018-05-31.
Nevertheless, the concept of DSP is neither intended to replace other stewardship concepts (in particular ASP) nor to be an alternative. DSP concerns decision making and goes beyond microbiological diagnostics alone. Kahneman et al. [2] said about decision making:
We think, each of us, that we’re much more rational than we are. And we think that we make our decisions because we have good reasons to make them. Even when it’s the other way around. We believe in the reasons, because we’ve already made the decision. [2]
Adequate diagnostics should help us to prevent this kind of situation in medicine by providing a basis to make well-informed decisions. Defining a proper diagnosis is a complex process with several aspects. We believe that DSP is a concept that requires collaboration between different medical specialties for optimal infection management and quality of care. This can include reduced morbidity and/or mortality, unnecessary interventions or treatments, complications, and length of stay. We want to point out why and how DSP affects the entire diagnostic process and that it involves more than just results or turnaround times of microbiological tests. By comparing different patient cases, we want to demonstrate how DSP serves the most important purpose: improved patient care. This involves process optimisation as a basis as well as medical questions and decisions on the individual patient level.
This entire diagnostic process requires multiple decisions along the way of patient care. Guidance and communication on this path are essential because:
Intuitive diagnosis is reliable when people have a lot of relevant feedback. But people are very often willing to make intuitive diagnoses even when they’re very likely to be wrong. [3]
Modern medicine is centred around evidence-based actions and tries to minimise the chance of mistakes while trying to keep the balance between the quality of care and the outcome on one hand and preventing collateral damage and costs on the other hand. In infection management stewardship activities can provide support and guidance in diagnosis and therapy. Physicians can be supported at the bedside to choose the right diagnostic test at the right time for the right patient. The same applies to therapeutic choices: the right treatment at the right time for the right patient in order to achieve the most optimal result. Naturally, these approaches to diagnostic and therapeutic support go hand in hand.
We outline two different case studies - fictitious but nevertheless realistic - of a patient with a prosthetic joint infection (PJI) in different scenarios and different outcomes. These examples underline how interdisciplinary stewardship can lead to a successful outcome for the patient and the physician.
2.1.1 Case 1
A 70-year-old woman was seen by the orthopaedic surgeon because of chronic pain in her hip prosthesis placed 3 years earlier. An X-ray showed signs of loosening of the prosthesis - an indication for revision surgery. C-reactive protein (CRP) was low (6 mg/L). The diagnosis of aseptic loosening was made, and the patient underwent revision surgery. To rule out low-grade infection, antibiotic prophylaxis was administered only after intraoperative tissue biopsies had been taken for culturing and histology. Cutibacterium acnes (formerly Propionibacterium acnes) was isolated from one out of five tissue biopsies (semi-quantitative <1+). Histology showed no indication of inflammation. The positive culture was considered contamination by the attending clinical microbiologist and the patient was discharged without further antibiotic therapy. However, during outpatient follow-up, the patient complained about persistent stiffness of her hip. Three years later, the patient presented again with recurrent loosening of the prosthesis and the presence of a fistula around the surgical site. A second revision intervention was necessary. Due to poor bone quality and poor soft tissue, multiple revisions were needed. Multiple intraoperative tissue biopsies revealed Cutibacterium acnes with the same antibiogram as three years earlier together with a methicillin-sensitive Staphylococcus hominis. The patient was given a cement spacer which made her temporarily immobile and was treated with a high dose of flucloxacillin intravenously. She was discharged with clindamycin per os and re-admitted several months later for reimplantation of the definitive prosthesis. After eight months of revalidation the functional result was poor. The patient permanently walks with support of a cane.
Figure 2.2 shows the course of the disease of this patient in which the decision moments are shown in circles. The potential stewardship zone shows the moments when a different action could/should have been taken.
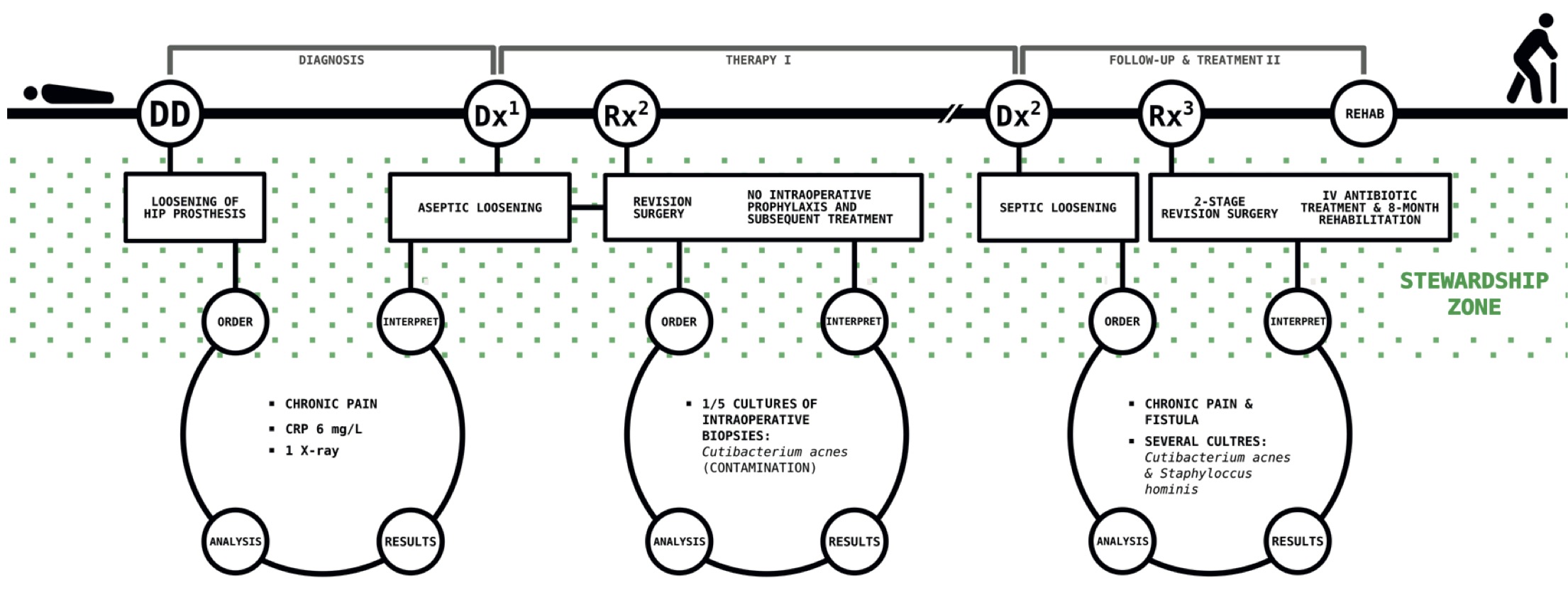
Figure 2.2: The first case.
The outcome for this patient was certainly not optimal. To illustrate how infection management with stewardship elements can improve the quality of care, a second case of the same patient with a PJI follows. Several additional diagnostic steps were performed (shown in bold) underlining the need for collaboration in stewardship activities including antimicrobial stewardship, of course, and how this affects clinical outcome and hospitalisation.
2.1.2 Case 2
A 70-year-old woman was seen by the orthopaedic surgeon because of chronic pain in her hip prosthesis placed 3 years earlier. An X-ray showed signs of loosening of the prosthesis - an indication for revision surgery. C-reactive protein (CRP) was low (6 mg/L). The radiologist was consulted to reassess the X-ray taken a year earlier. This image already showed subtle signs of radiolucency around the head and neck of the prosthesis making a mechanical cause of detachment less likely. Synovial fluid was punctured to rule out septic loosening of the prosthesis. The synovial fluid culture remained negative and the leukocyte count was only slightly increased, but several biomarkers were positive suggesting infection (450 mg/L calprotectin and positive alpha-defensin). Subsequently, prior to revision surgery, several tissue biopsies were taken by the orthopaedic surgeon in a sterile environment. Cutibacterium acnes (formerly Propionibacterium acnes) was isolated from one out of five tissue biopsies (5-10 CFU/ml). Histology showed no indication of inflammation. During revision surgery, antibiotic prophylaxis was given prior to surgical incision and several tissue samples were taken for culturing (including sonication) of the prosthesis. Empirical treatment was initiated with high doses of amoxicillin. Due to the previous positive culture with Cutibacterium acnes, all intraoperative cultures were incubated for 14 days on the advice of the clinical microbiologist. C. acnes was found again in two of five tissue biopsies and also in the sonication fluid. These isolates showed the same antibiogram as the isolates from before revision surgery. The patient was then discharged and treated at home with 10 weeks of amoxicillin per os. She fully recovered within a few weeks.
Figure 2.3 shows the additional decisions compared to Figure 2.2. These lead to a better outcome for the patient through the implementation of stewardships. The differences with Figure 2.2 are shown in red.
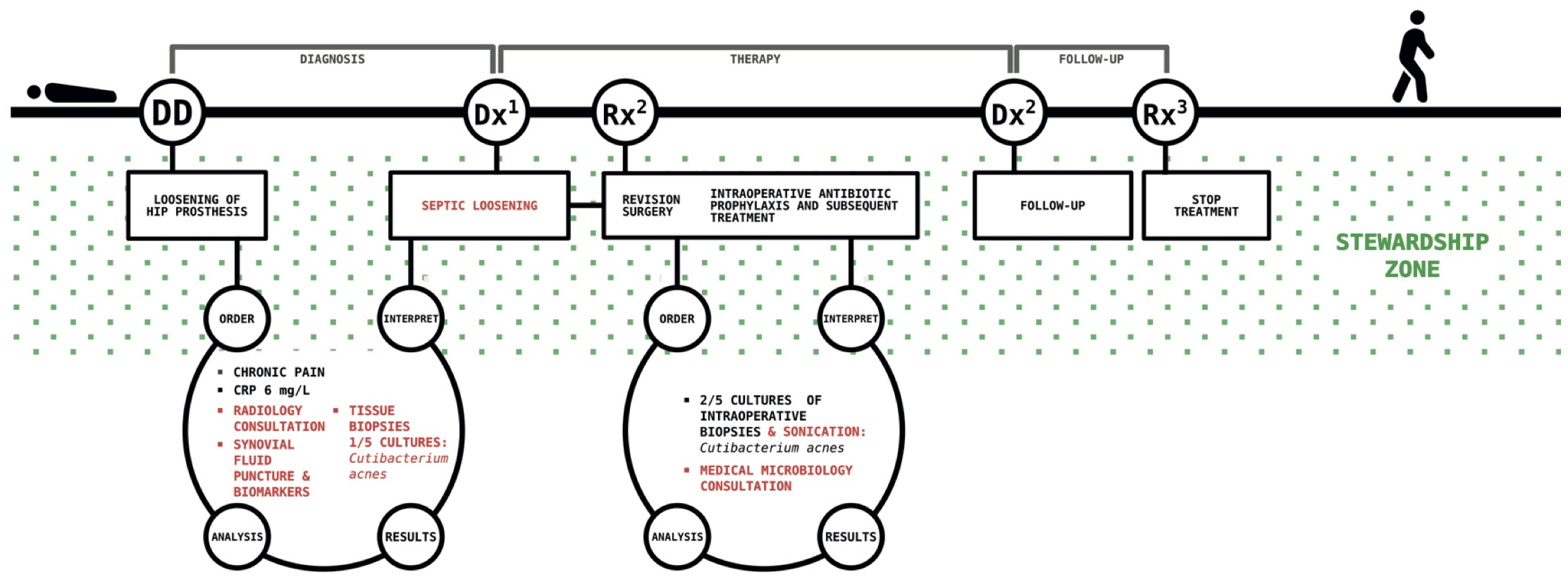
Figure 2.3: The second case.
2.2 The general concept
2.2.1 ‘Diagnostics’
The term diagnostics seems simple, but its various aspects are very diverse, as the cases above demonstrate. The second case emphasises the importance of stewardships and centres around facilitating an optimal care process through communication, crossing the boundaries of specialisms, and increasing awareness of the integral nature of successful infection management and optimal quality of care. Different physicians (involved in infection management) and their perceptions are reflected in this view on diagnostics. While some think of the entire process of diagnosing a disease, others think purely of the technical aspect in the lab as diagnostics (of their own speciality). This diversity underlines the importance of communication and collaboration across the boundaries of different medical specialties. The concept of stewardship is widely used to facilitate communication (and clinical decision making). Multiple attempts have been made to establish a clear definition of stewardship, but this has proved challenging [3,4]. Overall, most of these attempts have been made in the light of antimicrobial stewardship programmes (ASP) and are accompanied by terms such as responsibility, balance, due diligence, and management [3,4].
2.2.2 DSP in the microbiological laboratory
A medical laboratory usually only has added value if, in addition to the reporting and advice, the range of tests and the test technique meet the requirements of the applicant. The technical aspect of the medical microbiology laboratories has seen tremendous technological advances in recent years. Advanced developments such as sequencing as part the routine to identify isolate properties (e.g., resistance genes) and Matrix-Assisted Laser Desorption/Ionization Time of Flight (MALDI-TOF) mass spectrometry methods have recently revolutionized the laboratories [5-7]. In addition, many new and fast diagnostic assays such as point-of-care test (POCT) and molecular rapid diagnostic test (mRDT) have entered the market [8]. The progress is undeniable although integration into workflow, quality control, data storage and availability, added value, and clinical impact often still need to be evaluated.
We embrace these developments but there are two aspects that are really essential for optimal quality of care. Both these aspects can be achieved through stewardship. Firstly, stewardship provides guidance for the appropriate choice of a customised diagnostic strategy for individual patients and patient groups in a specific setting. Guidelines and protocols for diagnostic and appropriate therapeutic choices are key elements in the development of this guidance or steering. A stewardship framework can form the basis for personalised decisions in individual patient care. It has already been demonstrated that new tests such as the aforementioned mRDT are most cost-effective for the diagnosis of bacteraemia when combined with an antimicrobial stewardship programme [9]. In addition, mRDT is associated with a significant reduction in mortality risk for septic patients but only when combined with ASP [10].
Secondly, it is important to consider the entire information loop in a process-oriented way and not just focus on the time-to-result. Stewardship covers this loop and starts making choices at the bedside. In addition, the interpretation of test results and timely feedback are equally important in order to be able to make good, evidence-based, and rapid therapy adjustments when needed. For example, physicians considering starting non-prophylactic intravenous antimicrobial treatment should (almost) always take blood cultures before starting. Although this is standard care and described in international guidelines [11], compliance is only 30 to 50% [12, 13, Luz et al.; unpublished data]. Only through complete ‘loops,’ from bedside to bedside, can better technology and improved work processes in microbiology laboratories be extended and made to work to their full potential.
2.2.3 DSP as process optimisation
Turnaround times (TAT) are a commonly used but poorly defined term in many areas. In a systematic review, a total of 61 different TAT definitions (out of a total of 151) were found to be used in several clinical areas [14]. Of those, only 10 definitions cover the time from test order placement to the time at which the results are being viewed by the ordering physician (Figure 2.4).
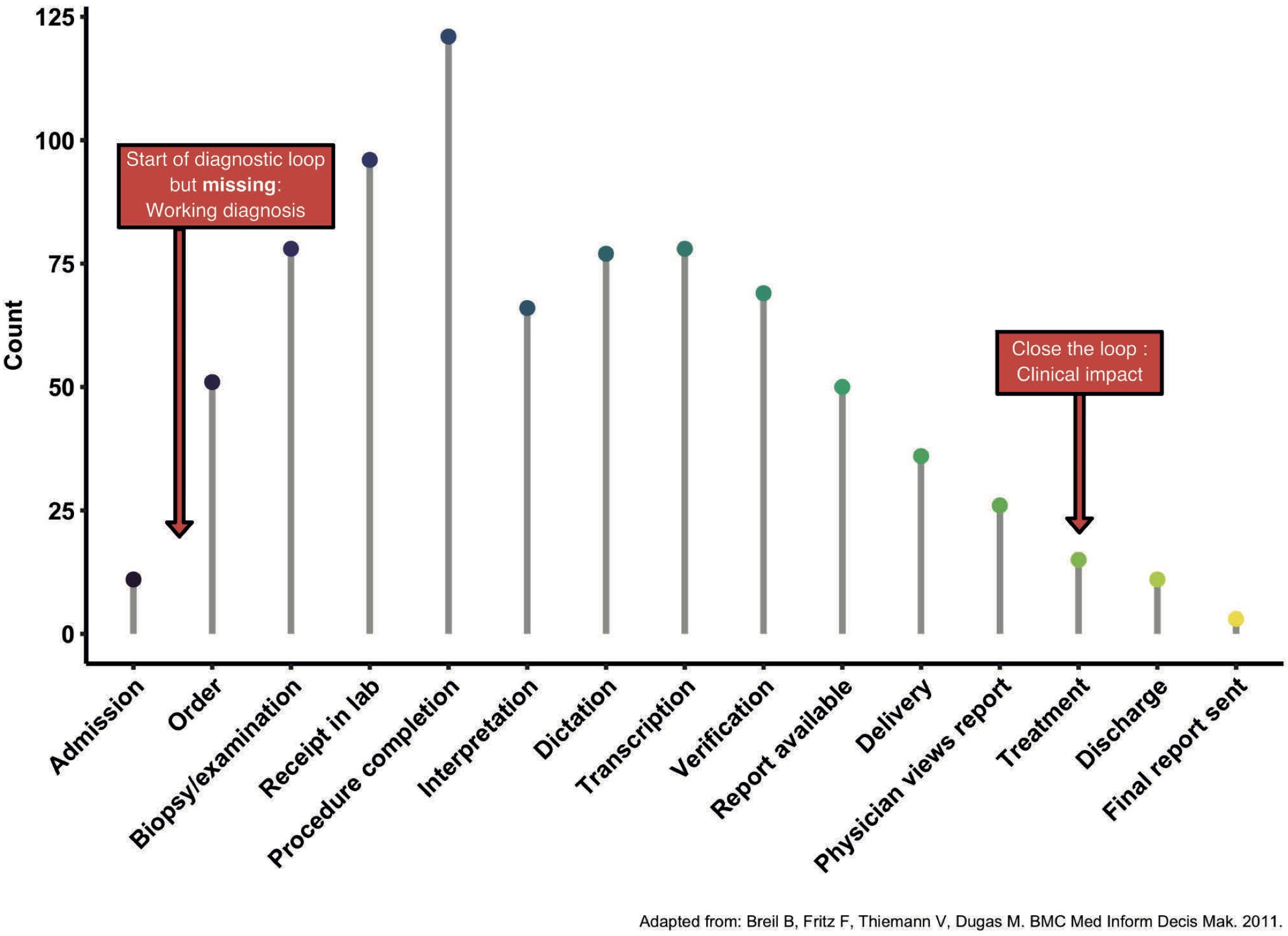
Figure 2.4: Time points mentioned in TAT definitions.
Nevertheless, even the order of a test is a decision within a diagnostic loop and should be taken into account when time is measured. We are convinced that infection management can help to understand the importance of a full loop from moment of choice to moment of choice, from the bedside to a diagnostic result and back. This implies the time from the moment when the need for diagnostics becomes clear, to the time when it can be acted upon based on its results. We call this time to action which is indicated by a red arrow in Figure 2.4.
2.2.4 Multidisciplinary aspects of DSP and infection management
It is essential to realise that the information needed to assess this time to action does not come only from microbiological laboratories. Communication and collaboration in the stewardship zone (Figures 2 and 3) are key and this applies to all specialities. But what would be the effect on the patient if microbiological diagnostics were not led by DSP when there is already good communication and cooperation in place? Would DSP no longer be necessary? Or is good cooperation equivalent to DSP?
DSP can significantly reduce the time to action by making proper use of each other’s expertise to make optimal decisions for the patient. In practice, information from one diagnostic discipline can help to steer the diagnostic process of another diagnostic discipline. One reason for this is that during the diagnostic process of many disciplines, such as medical microbiology and imaging, an intrinsic amount of interpretation takes place. The clinical course is no less important here. We always need DSP, because together we try to act as optimally as possible in the interest of the patient, in which diagnosis is an important tool. DSP is not specific to medical microbiology, as demonstrated by the relevance of its collaboration with radiology in case 2. Nor is it specific to any other speciality. DSP is not intended as a reactive ad hoc solution but rather as a proactive, structural approach. DSP should be seen as guiding the entire diagnostic process, not only on the basis of antibiotics, but also on the basis of extensive imaging (such as for endocarditis), biomarkers (such as leukocytes and CRP, or procalcitonin for de-escalation of treatment), or by therapeutic drug monitoring (TDM) modelling the optimal dosage from the start of (empirical) treatment for individual patients and patient groups. One form of diagnostics is relevant to monitor trends, the other to directly answer a clinical question. This does not mean that one is less important than the other or that we should look at the value of an antibiogram differently from the value of a therapeutic drug monitoring. A pharmacist is also part of DSP.
As an example, in Dutch hospitals we are used to having a hospital pharmacist in house, providing clinical pharmaceutical services. Consultations are typically performed via e-mail, telephone, or an electronic prescription system. On the other hand, in countries such as the United Kingdom, these pharmacists work in infection management in the clinical (nursing) departments on a daily basis in collaboration with other specialists. This supports the most safe, appropriate, and cost-effective antimicrobial treatment [15]. In addition, as mentioned earlier, the guidance of antimicrobial therapy by TDM is another important aspect. Hospital pharmacists can make suggestions on sample timing for TDM, inform about early prediction of attainable levels and dose adjustments to achieve adequate exposure and reduce toxicity as quickly as possible, and interpret results [16]. As a result, they are an integral part of the stewardship concept. We are convinced that the different stewardship terms and concepts form synergy for the best infection management [1,17]. Infection management has different aspects (such as ASP) and stewardship refers to guidance provided by focused experts [18].
Empirical antimicrobial therapy is a good example to illustrate how these aspects are linked. The working diagnosis (see also cases 1 and 2), based on an appropriate differential diagnosis, forms the basis for an appropriate empirical therapy that takes into account the most relevant pathogens, their anticipated susceptibility, the source of infection (taking into account the compartment), and underlying patient factors. Adequate initial diagnostic initiatives (such as deep focus puncture, see case 2) may simultaneously be therapeutic (such as surgical/interventional drainage for source control). Vice versa, the clinical course under therapy can be diagnostic in itself, for example, if diagnostics for the working diagnosis are correct and complete. Ultimately, the treatment of patients with complex infections almost always requires targeted treatment. This, in turn, requires adequate initial and ongoing diagnostics for optimal treatment. Figure 2.5 shows the decision moments and different specialisms that can be involved in this whole process.
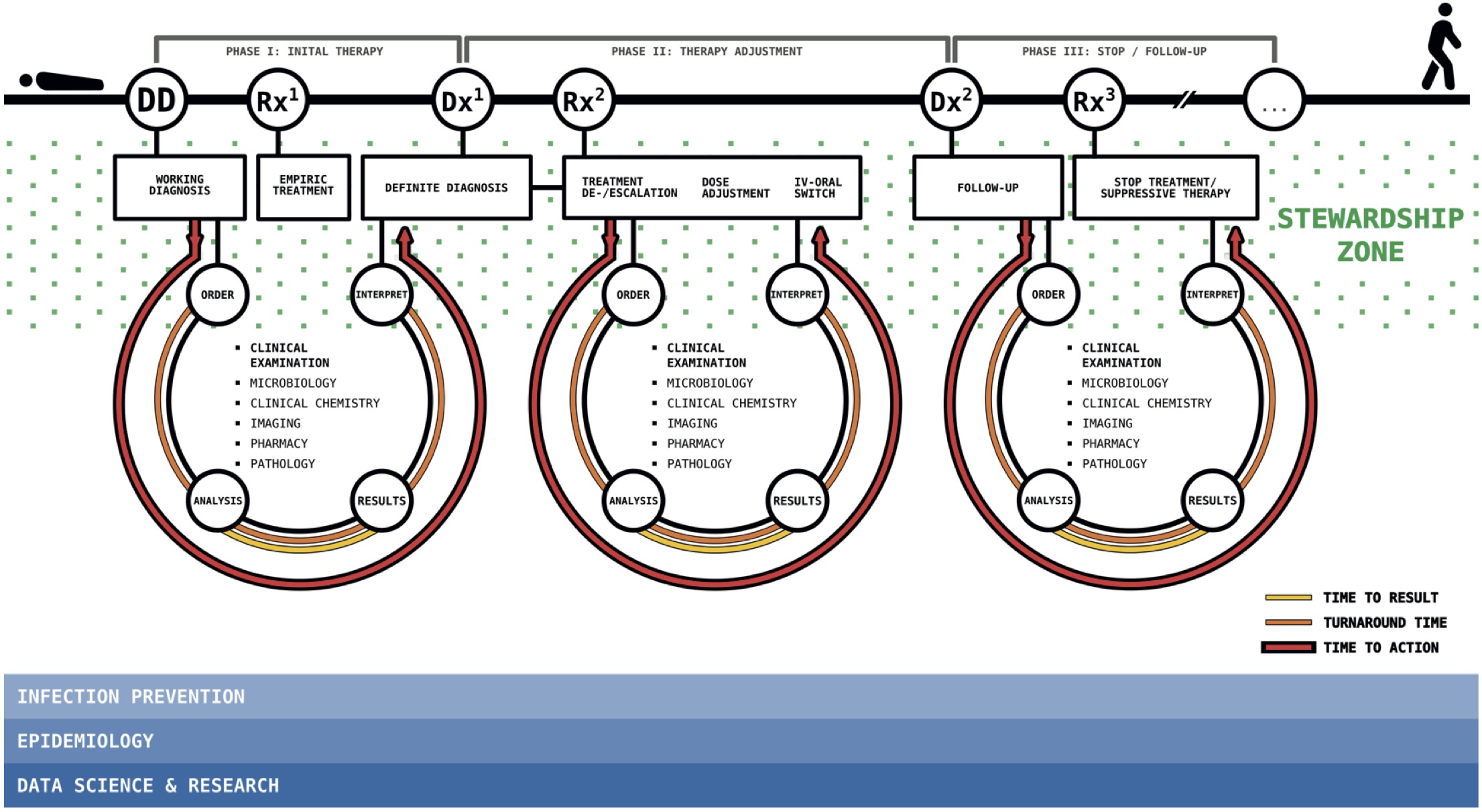
Figure 2.5: Stewardship in infection management.
2.3 Conclusion
The answer to the question from the title (Diagnostic stewardship - sentence or nonsense?!) is: both. It is nonsense to debate terminology and the discussion about differences between diagnostic stewardship and infection management is only of semantic nature. Diagnostic stewardship makes sense in the concept discussed above. It can guide specialists (physician-microbiologist/medical-molecular microbiologists and experts from other fields, such as hospital pharmacists, radiologists, nuclear medicine, etc.) to the area of the stewardship zone of interaction and communication (Fig. 5), where they can bring in their expertise to complex clinical decision-making. Clinical information, including a patient’s clinical development, is extremely important for correctly interpreting diagnostic results and steering the process. It can also help leading clinicians and other clinicians to understand the full potential (and limitations) of diagnostics and how important they are for evidence-based decision-making. We follow an integrated stewardship model that adds different perspectives (antimicrobial, infection prevention, and diagnostic stewardship - AID) to the ultimate goal of all stewardship intentions - the best quality care for the individual patient [1].
Stewardship consists largely of translation and communication during the decision-making process. Diagnostics are essential in this. But there is no need for a new name. Diagnostic stewardship as a name may be without added value and more and more use of stewardship-like terms could lead to confusion. The aim of all efforts and experts in infection management is the same: to improve quality of care and patient outcomes. We see with our own eyes how DSP guidelines are adhered to and realise how important it is that we continue to emphasise the often-underexposed diagnostic aspects of infection management. Multidisciplinary management based on diagnostics builds the basis for optimal outcomes for patients with infections.
Financing
This study was partly supported by the INTERREG V A (202085) funded project EurHealth-1Health (http://www.eurhealth1health.eu), part of a Dutch-German cross-border network supported by the European Commission, the Dutch Ministry of Health, Welfare and Sport, the Ministry of Economy, Innovation, Digitalisation and Energy of the German Federal State of North Rhine-Westphalia and the Ministry for National and European Affairs and Regional Development of Lower Saxony.
In addition, this study was part of a project funded by the European Union’s Horizon 2020 research and innovation programme under the Marie Sklodowska-Curie grant agreement 713660 (MSCA-COFUND-2015-DP “Pronkjewail”).
References
- Dik J-WH, Poelman R, Friedrich AW, Panday PN, Lo-Ten-Foe JR, van Assen S, et al. An integrated stewardship model: antimicrobial, infection prevention and diagnostic (AID). Future Microbiol. 2016;11(1):93–102.
- Kahneman D. Thinking, fast and slow. Macmillan; 2011.
- Dyar OJ, Huttner B, Schouten J, Pulcini C, ESGAP (ESCMID Study Group for Antimicrobial stewardshiP). What is antimicrobial stewardship? Clin Microbiol Infect. 2017 Nov;23(11):793–8.
- Mendelson M, Balasegaram M, Jinks T, Pulcini C, Sharland M. Antibiotic resistance has a language problem. Nature. 2017 May 3;545(7652):23–5.
- Greub G, Moran-Gilad J, Rossen J, Egli A, ESCMID Study Group for Genomic and Molecular Diagnostics (ESGMD). ESCMID postgraduate education course: applications of MALDI-TOF mass spectrometry in clinical microbiology. Microbes Infect. 2017 Sep;19(9-10):433–42.
- Didelot X, Bowden R, Wilson DJ, Peto TEA, Crook DW. Transforming clinical microbiology with bacterial genome sequencing. Nat Rev Genet. 2012 Sep;13(9):601–12.
- Greninger AL. The challenge of diagnostic metagenomics. Expert Rev Mol Diagn. 2018 Jun 18;1–11.
- Kozel TR, Burnham-Marusich AR. Point-of-Care Testing for Infectious Diseases: Past, Present, and Future. J Clin Microbiol. 2017 Aug;55(8):2313–20.
- Pliakos EE, Andreatos N, Shehadeh F, Ziakas PD, Mylonakis E. The Cost-Effectiveness of Rapid Diagnostic Testing for the Diagnosis of Bloodstream Infections with or without Antimicrobial Stewardship. Clin Microbiol Rev. 2018 Jul;31(3).
- Timbrook TT, Morton JB, McConeghy KW, Caffrey AR, Mylonakis E, LaPlante KL. The Effect of Molecular Rapid Diagnostic Testing on Clinical Outcomes in Bloodstream Infections: A Systematic Review and Meta-analysis. Clin Infect Dis. 2017 Jan 1;64(1):15–23.
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit Care Med. 2017 Mar;45(3):486–552.
- Reissig A, Mempel C, Schumacher U, Copetti R, Gross F, Aliberti S. Microbiological diagnosis and antibiotic therapy in patients with community-acquired pneumonia and acute COPD exacerbation in daily clinical practice: comparison to current guidelines. Lung. 2013 Jun;191(3):239–46.
- Shallcross LJ, Freemantle N, Nisar S, Ray D. A cross-sectional study of blood cultures and antibiotic use in patients admitted from the Emergency Department: missed opportunities for antimicrobial stewardship. BMC Infect Dis. 2016 Apr 18;16:166.
- Breil B, Fritz F, Thiemann V, Dugas M. Mapping turnaround times (TAT) to a generic timeline: a systematic review of TAT definitions in clinical domains. BMC Med Inform Decis Mak. 2011 May 24;11:34.
- Wickens HJ, Jacklin A. Impact of the Hospital Pharmacy Initiative for promoting prudent use of antibiotics in hospitals in England. J Antimicrob Chemother. 2006 Dec;58(6):1230–7.
- van Wanrooy MJP, Rodgers MGG, Span LFR, Zijlstra JG, Uges DRA, Kosterink JGW, et al. Voriconazole Therapeutic Drug Monitoring Practices in Intensive Care. Ther Drug Monit. 2016 Jun;38(3):313–8.
- Pulcini C, Binda F, Lamkang AS, Trett A, Charani E, Goff DA, et al. Developing core elements and checklist items for global hospital antimicrobial stewardship programmes: a consensus approach. Clin Microbiol Infect [Internet]. 2018 Apr 3; Available from: http://dx.doi.org/10.1016/j.cmi.2018.03.033
- British Society for Antimicrobial Chemotherapy. Antimicrobial Stewardship: From Principal to Practice [Internet]. Birmingham, United Kingdom: British Society for Antimicrobial Chemotherapy; 2018. Available from: http://bsac.org.uk/antimicrobial-stewardship-from-principles-to-practice-e-book/